Oct 11, 2024 - KFF
On October 8, 2024, Vice President Harris proposed to expand Medicare to provide home care to help families who are struggling with the costs of long-term care. If enacted, this would be the first major expansion of Medicare since the Medicare Modernization Act of 2003 that added a prescription drug benefit to the program.
Vice President Harris proposes to create a new home care benefit for eligible Medicare beneficiaries. Under the proposal, Medicare beneficiaries would be eligible for the new benefit if they are unable to perform activities of daily living such as bathing and eating or have a serious cognitive impairment, such as Alzheimer’s disease. Although the proposal is not fully specified, it “recognizes that the vast majority of seniors with long-term care needs are still able to live in their homes with an average of 20 hours or less a week of care,” suggesting that the benefit will be around 20 hours per week. The new benefit includes cost sharing requirements that vary by income. The proposal notes that similar home care proposals have been estimated to cost about $40 billion per year, prior to accounting for potential savings from reduced use of hospital and nursing facility care.
In addition, the proposal would expand Medicare to cover vision and hearing, and end a practice known as “estate recovery” when Medicaid recoups the costs of home care from the sale of decedents’ homes and estates (described below). The proposal would fund the additional costs of the new benefits by expanding Medicare drug negotiation provisions included in the Inflation Reduction Act; increasing the discounts covered by drug manufacturers for certain brand-name drugs; strengthening requirements for pharmacy benefit managers related to price transparency and competition; and by implementing international tax reforms.
KFF estimates that 14.7 million Medicare beneficiaries (23% of those living in the community) would potentially be eligible for the new Medicare home care benefit. This estimate is based on eligibility criteria used in similar proposals: having two or more limitations in activities of daily living and/or a serious cognitive impairment. The number of people eligible for this benefit could be higher or lower depending on how eligibility criteria are defined, and not all people who are eligible for the program will use the new benefits. This estimate is based on an analysis of the 2022 Medicare Current Beneficiary Survey and excludes beneficiaries living in nursing homes and other long-term settings (see Methods).
Former President Trump has endorsed “at home Senior Care” but has not put forward a specific proposal. Former President Trump proposes “shifting resources back to at-home Senior Care,” addressing disincentives that contribute to workforce shortages, and supporting unpaid family caregivers through tax credits. It’s unclear whether the Trump proposals would apply to people with disabilities who use home care, if they would make changes to Medicare or Medicaid, or how they align with broader proposed cuts to the Medicaid program. Although Vice President Harris’ fact sheet focuses on older adults, the proposal would expand Medicare, which includes both adults ages 65 and older and younger adults with disabilities, suggesting that Medicare beneficiaries with disabilities would also be eligible for the new benefit.
Under current law, Medicare coverage of home care is quite limited. Medicare covers home health aide services for people who need skilled services on a part-time or intermittent basis, such as nursing or physical therapy, and are “homebound.” Because of the skilled care requirement, Medicare does not cover home care for many people who need help on an ongoing basis due to limitations in activities of daily living or cognitive impairments, but don’t also require skilled services.
Medicaid pays for two-thirds of all spending on home care in the U.S., but coverage rules are complex and coverage is for people with limited financial resources. Most home care services in Medicaid are provided at the option of states, and optional services result in variability of available benefits. Roughly 700,000 are on waiting lists for home care because the number of people seeking services exceeds the number of people states can serve.
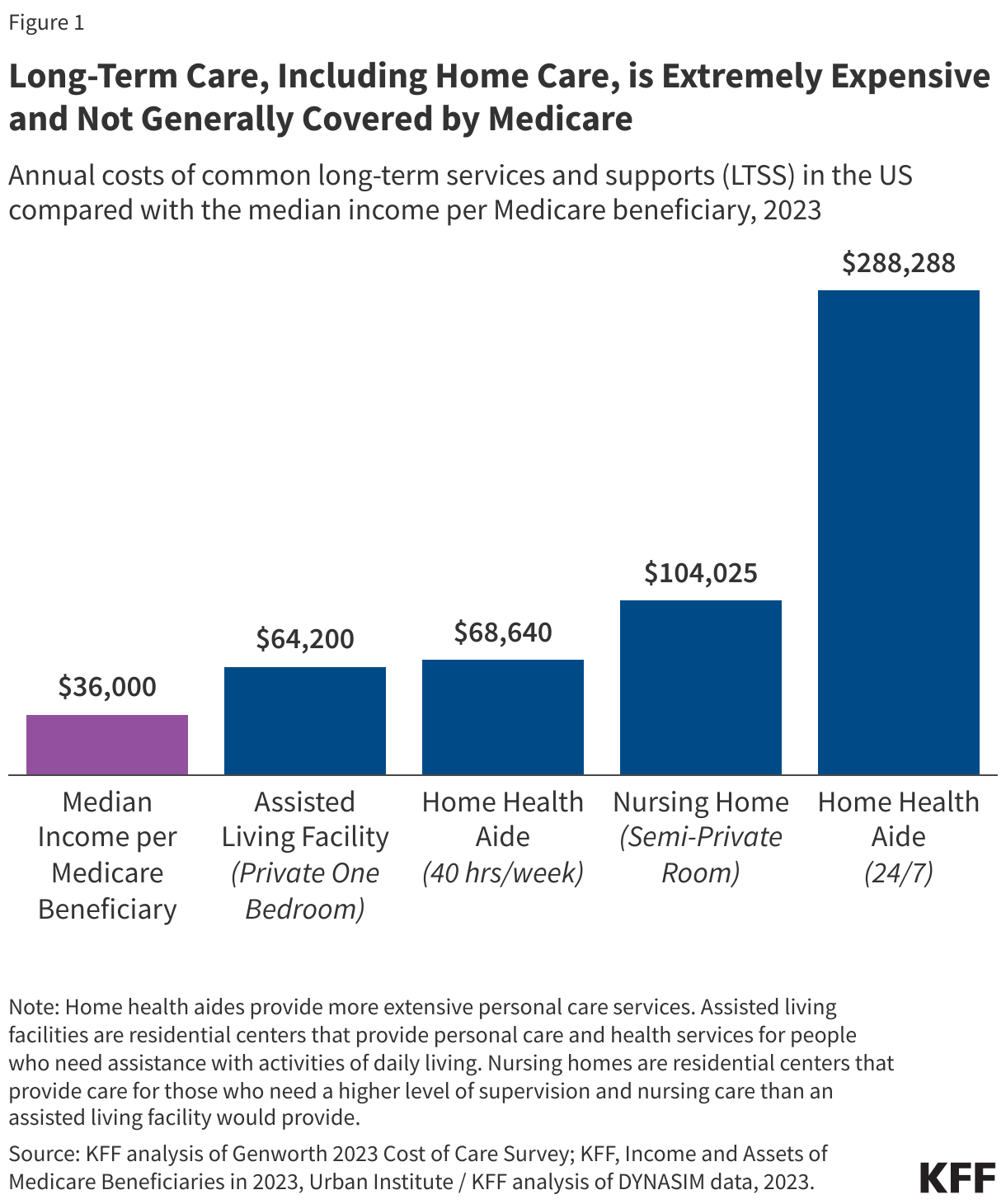
People who need home care and other long-term care services often pay substantial amounts out-of-pocket (see Figure 1). Those costs often exceed the median income for Medicare beneficiaries (about $36,000 per beneficiary in 2023) and may quickly exhaust the median savings ($103,800 per beneficiary in 2023). KFF polling finds over half of all people who used long-term care or paid for a family member’s care reported having to reduce their spending on food, clothing, or basic household items as a result of these costs.
Vice President Harris’ proposal would also expand Medicare to cover vision and hearing. Under current law, traditional Medicare does not cover prescription eye wear (eyeglasses/contacts) or hearing aids, which can be prohibitively expensive for people living on fixed incomes. Difficulty with hearing and vision is relatively common among Medicare beneficiaries, with close to half (44%) of beneficiaries reporting difficulty hearing and more than one third (35%) reporting difficulty seeing in 2019. Limited hearing and vision benefits are typically offered by Medicare Advantage plans but the scope, value and provider networks of these benefits varies widely across plans. Beneficiaries in traditional Medicare may have access to some hearing and vision benefits if they also have supplemental coverage under Medicaid, employer or union-sponsored retiree health benefits, or other types of insurance.
Beyond changes to Medicare, Vice President Harris is proposing to end a practice in which Medicaid recoups the costs of home care from the sale of decedents’ homes and estates. Under Medicaid estate recovery, states are required to recoup the costs of long-term care and related hospital and prescription drug services for Medicaid enrollees ages 55 and older, and have the option to recover the costs for other services and populations. The Harris proposal proposes to work with Congress to end Medicaid estate recovery or use administrative action to expand the circumstances in which families may be exempted, if Congress fails to take action.
Estate recovery practices have been criticized for several reasons, including that it falls primarily on individuals with limited incomes, raises little revenue, and is applied very unevenly across the states. Democrats have recently proposed eliminating estate recovery while Republicans have recently proposed modifying the rules and prohibiting it under certain circumstances.
Nearly all provisions in Vice President Harris’ proposal would require a change in law. Without Congressional action, a new Administration would be unable to establish and fund new Medicare benefits for home care, vision, and hearing; generate savings by enacting changes to the Inflation Reduction Act’s Medicare prescription provisions; eliminate Medicaid estate recovery; or establish new taxes. Both Democrats and Republicans have proposed legislation to reduce the number of people waiting to receive Medicaid home care and address the issue of Medicaid estate recovery, suggesting that may be an area of potential compromise. There is also bipartisan interest in beefing up oversight and transparency for pharmacy benefit managers (PBMs).
As the proposal winds its way through Congress, many policy details would have to be worked through. For example, in addition to laying out more specifics about how to fully fund the benefit expansions, lawmakers would face questions about how eligibility for the new benefits would be determined; who could be paid to provide the new benefits; and how the new benefits would interact with existing Medicare benefits, and with supplemental coverage provided through Medicaid or private policies. Lawmakers would also likely debate how to support care workers, improve their wages, and address ongoing workforce shortages in the home care industry. The answers to these and other questions would impact how many people would be helped and the cost.
The proposal includes a small number of changes that could be enacted without new legislation, such as strengthening requirements for pharmacy benefit managers related to price transparency and competition and expanding the circumstances in which families may obtain exemptions from Medicaid estate recovery.
Methods |
| This analysis uses the Centers for Medicare & Medicaid Services’ Medicare Current Beneficiary Survey (MCBS), 2022 Survey File (the most recent year available) to obtain data on the number and share of Medicare beneficiaries who would potentially be eligible for the proposed home care benefit. The analysis assumed that Medicare beneficiaries with either two or more limitations in activities of daily living (ADLs) or a cognitive impairment would be eligible. The MCBS is a nationally representative survey of Medicare beneficiaries.
The analysis is limited to community-dwelling Medicare beneficiaries and excludes beneficiaries who live in long-term care or other residential facilities such as skilled nursing facilities or assisted living facilities. For Medicare beneficiaries in the community, cognitive impairment is defined as at least one positive response to:
Medicare beneficiaries in the community were defined as potentially eligible for the proposed home health care benefit if they reported difficulty performing two or more of the following ADLs because of a physical, mental, emotional, or memory problem: bathing or showering, getting in or out of bed or chairs, dressing, eating, using the toilet (including getting up and down), or walking. These difficulties may have been temporary or chronic at the time of the survey. |